limited Transthoracic ECHOCARDIOGRAPHY
Views and Anatomy
Parasternal Long Axis views
Parasternal long axis - standard view
Parasternal Long Axis - RV inflow view
Parasternal Long Axis - RV Outflow view
-
Start with cardiac/phased array/sector probe
Set machine to cardiac preset
Hold probe like a pencil
Place probe on patient’s left chest, just left to the sternum around the 3rd - 5th intercostal spaces. Add firm pressure and feel the probe shift into an intercostal space.
Orient probe maker to patient’s right shoulder (long-axis view)
While watching the screen, start moving the probe in small circles from this point slowly spreading out in all directions, making larger movements as you go. Watch the screen the entire time and look at the heart as it comes in and out of view as you pass over ribs and lung.
Identify the best cardiac window and anchor the probe. Add firm pressure and feel the probe shift into the intercostal space. Stabilize your position by placing your wrist on the patient’s body.
To fully optimize the view, make slow deliberate movements with slight changes in angle (North/South/East/West) and rotation (clock/counter-clock) in all directions. “Mortar and pestle movements”
Focus the mitral value leaflets at the center of the screen and rotate clockwise or counter-clockwise to open up the LVOT.
parasternal short axis - apical view
How to Parasternal Short Axis Views
Start from the optimal parasternal long axis window and view
Rotate probe 90 degrees clockwise (dot toward left shoulder)
This will likely result in a short axis view at the mitral valve level.
The optimal technique in a normal patient will provide a cleanly round LV. In order to fully optimize the view, make slow deliberate movements with slight changes in angle (North/South/East/West) and rotation (clock/counter-clock) in all directions. “Mortar and pestle movements”
Angle or slide the probe toward the cardiac base or apex to visualize the following:
Base of heart at level of aortic valve (medial and angle toward base
Mitral valve level
Papillary Level
Apical Level
Tips For The Novice POCUS Provider (see section below)
Practice Parasternal



Apical Anatomy and Views
How to apical 4 & chamer view
Start with cardiac/phased array/sector probe
Set machine to cardiac presets
Hold probe like a pencil
Roll patient on left lateral decubitus (for patients that will tolerate rolling)
Place probe on patients left lateral chest at approximately the 5th intercostal space located just below the nipple in men and that left breast in women. You should add firm pressure and feel the probe shift into an intercostal space.
Orient probe maker toward patient’s left axilla
Be sure that the probe is angled shallowly, trough the apex of the heart toward the base. The probe handle should be low and pointed to left hip.
While watching the screen, start moving the probe in small circles from this point slowly spreading out in all directions. Watch the screen the entire time and look at the heart as it comes in and out of view as you pass over ribs and lung.
Identify the best cardiac window and anchor the probe. Stabilize your position by placing your wrist on the patient’s body.
To fully optimize the view, make slow deliberate movements with slight changes in angle (North/South/East/West) and rotation (clock/counter-clock) in all directions. “Mortar and pestle movements”
Focus the left ventricular apex at the top of the screen and bring septum to the middle of the screen in a vertical orientation. (see figure 2a)
Tips For The Novice POCUS Provider (see section below)
Subcostal anatomy and Views

Additional scanning Tips

***COPD/obstructive lung disease will shift the heart to lower position in thorax
***Body size may greatly affect position of heart and ability to achieve optimal views. Tall and thin patients will often have a medially place apex.
***Be aware that the heart may come in and out of view with respirations. Slow movements will allow the scanner to find the correct window. One useful technique is to have the patient arrest breathing at various times during inhalation and exhalation to find the optimal view. This technique can be very effective if the patient is able to cooperate and it is even more effective if the patient can see the screen.
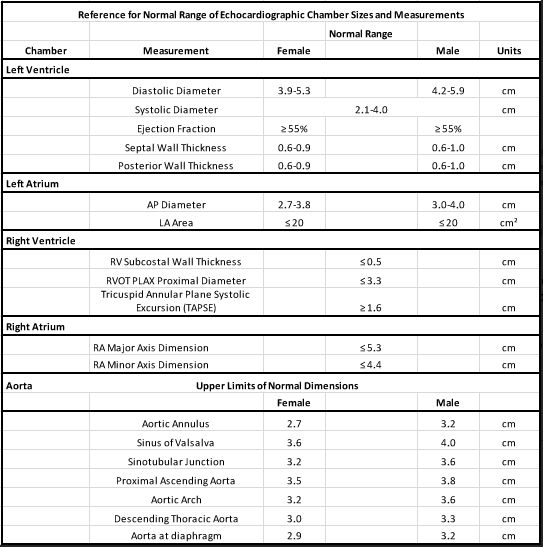
Basic Anatomic Measurements (1)



Apical views
Apical two chamber view
apical 3 chamber view
Apical four chamber view


apical Five Chamber View


Subcostal Views
Subcostal four chamber view
Subcostal Long
practice subcostal
References
(1) Otto, C. M. (2004). Textbook of clinical echocardiography / Catherine M. Otto. Philadelphia: Elsevier Saunders.
AUTHORS
MATT JONES, MD
SEAN WHITTY, MD CANDIDATE CLASS OF 2020
CONSULTant
DON BYARS, MD (emergency medicine)